
Understanding Risk From Viral Disease
Infection is a risk factor, not a disease
A century ago, an influenza virus, nicknamed the Spanish flu, killed 50 million people over two years. It was the most deadly viral pandemic in recorded human history. How did this pandemic end?
It hasn’t ended— at least not if we apply the same metrics used in current news reports and government policies to judge success with COVID-19. The Spanish flu got rebranded as a member of the seasonal flu a long time ago. But the virus formerly known as Spanish flu is still causing seasonal outbreaks to this day. People are getting infected and reinfected multiple times in their lives. Individuals in high-risk groups are dying from Spanish influenza today, a century after the pandemic began and decades after a vaccine was available.
No expert would say that the 1918 pandemic was still ongoing. Something strange happened this year. Our leaders changed the rules for COVID-19. Politicians, journalists, even some scientists started to compute risk and quantify harm from this latest viral disease differently than we had for any previously existing virus or any human illness. We began counting infections, not disease, as the metrics of success for a public health policy.
Infections are a risk factor for a viral disease, not the disease itself. We are making a category error. The vast majority of viral infections do not cause disease. Most infections help prevent future illnesses. These new metrics set the acceptable risk level from the viral disease so low it cannot be reached with any modern medical treatments or tools. That's not progress. That’s fear-mongering.
Viruses don’t go away. The numbers we are reporting and decisioning on right now—infection rates, daily percentage of positive tests—-these numbers will never stay low enough to prevent shutdowns for any significant time, even years from now. This coronavirus will be recurring in seasonal waves for the rest of our lives.
Epidemiologists never counted infections as a problem itself before 2020. Remember swine flu? It made the news briefly in 2009. That’s the same strain of the virus that caused the Spanish flu. This novel and deadly virus caused a global pandemic only a decade ago. Yes, you have lived through other deadly global pandemics. Since 2009, a considerable percentage of the global population has been infected with this mutant of influenza, most unaware as it happened. Some of us did not have symptoms at all. A few of us felt tired one night, and that was a subtle sign of fighting off an infection we brushed off as work stress. Others thought it was a cold, a bad headache, or correctly labeled it the flu but not the new flu type. When young and healthy, we experience many viral infections as minor nondescript annoyances— like how the vast majority of the public experiences COVID-19 today.
Infection without disease is a common phenomenon in epidemiology. It is easy to find other examples that are less politically fraught than comparing COVID-19 to the flu. Only 1 in 4 people have had the kissing disease, mono, in their lifetime. But 90% of adults have immunity to the EBV virus that causes mono. If you never got mono during your teenage years, it is more likely than not that you had the infection without knowing it. You could have even been the super-spreader in your high school or college. We all infected each other as an age-appropriate social herd.
Measles is another top-of-mind example of infections regularly occurring without causing disease. Measles outbreaks recurred in the past five years. This recurrence was only possible because the measles virus was circulating and causing asymptomatic infections in our population. If the measles had been eradicated, it couldn’t have recurred even due to the anti-vax movement's nonsense.
Viral infections are ubiquitous, and that can be a good thing. Constant endemic minor infections prevent deadly pandemics from novel viruses, like a booster shot for a vaccination program. The swine flu pandemic of 2009 was nothing like the Spanish flu of 1918. Many people, specifically high-risk groups over 60 years old, were partially immune to the virus from childhood infections. If we had prevented these past infections, the swine flu pandemic would have been much more deadly within the high-risk population than it was.
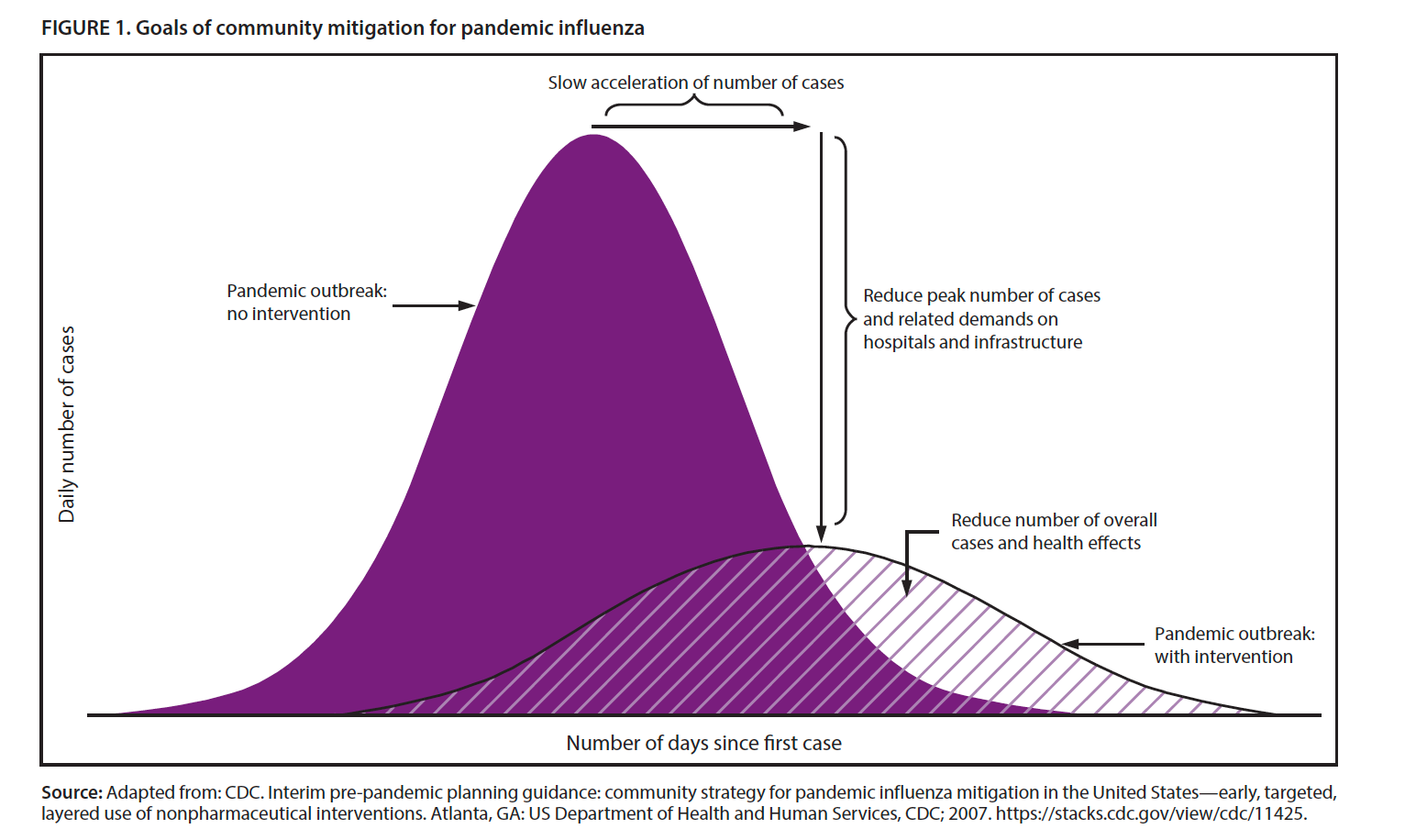
As we age, our immune system is less effective at fighting off infections. We experience more disease, or more severe forms of the disease, with each infection. Perhaps, we feel sick enough to go to the doctor instead of just shaking it off as stress-related exhaustion. That act, the choice to go to the doctor for treatment, is the official difference between a ‘case’ and ‘infection’ in usual public health metrics (see graph below). There are more cases of the flu in high-risk groups in our population, not necessarily more infections. The co-occurrence of the risk factor of age with the risk factor of infection is more likely to result in disease. Of course, age is a risk factor for most diseases. Our knees and backs hurt more from a tennis match at age 45 than when we played at 15. Our bodies ache more from the same infection, too—aging blows.
What about vaccines?
We can minimize harm from COVID-19 without preventing all underlying infections. That’s the only option we have available. Vaccines are not treatments for a viral disease. They use our immune system to prevent an infection from becoming a disease. One needs a functioning immune system for this to work. Low-risk groups historically respond well to vaccines but often had minimal disease risk to start. Vaccines are less effective in high-risk groups for the same reasons these groups are more susceptible to disease in the first place. We don’t have a cure for age.
At the population level, vaccines can eventually lower the number of infections. This reduction occurs through a process known as herd immunity. When the people around you, your social circle or herd, do a better job of fighting an infection in their own body, they are less likely to expose you to the virus in the first place. As we age, we rely even more on our family and friends—on herd immunity—to stay healthy.
The Wisdom to Know the Difference
Viruses never go away. Viruses never stop spreading. It doesn’t make sense to be afraid of SARS-COV-2 or to organize your life to avoid it. You are going to be infected eventually, even if you get a vaccine first. You do not have control.
Let’s address two common fears these days. First, fear that you are killing someone else by allowing yourself to get infected today. Second, fear of unknown consequences of viral infections.
Infections sometimes have long-term health impacts even without disease. I am unaware of examples from past coronaviruses or the common cold. I would bet money any claims of side-effects end up being bad science. But it is not impossible. HPV infections correlate with cervical cancer, and the EBV virus (mono) causes lymphoma and other cancers (~140,000 deaths each year). These risks are real, but about the same scale as thousands of other tiny risks inherent to human life.
As for blame, no one would say you killed your high-school boyfriend by kissing him decades ago, even if he eventually died from EBV+ lymphoma. Trying to optimize for a seventh-order consequence is not a viable way to live life or make risk-based decisions. Things in life are not that predictable, and many events are overdetermined (if it weren't one thing, it’d be another). Public health officials making this argument about COVID-19 should know better. This idea is central to risk management and taught in introductory classes in the field.
If you are healthy right now, the disease risk from a SARS-COV-2 infection is minimal. If you are in a high-risk group, please take extra precautions, not just for COVID-19 but for all infections and high-risk activities.
We are managing two major risk factors right now: the risk from infection and age. We cannot prevent infections. We are all getting older, no matter what we do. I hope one day to be in the high-risk group for respiratory infections. I may even die from COVID-19 or the Spanish flu one day. But that would mean I was lucky enough to live that long. We need to think more about what that means for how we define success.